What is slipped disc?
A slipped disc is also known as a herniated disc. A herniated disc is a displacement of disc material beyond the intervertebral space. It may cause pain over the area or associated with nerve root compression which refers to pain in the other area. The disc herniation is most common in the lumbar spine and the followed by the cervical spine as they are the flexible part of the spine.
The intervertebral disc consists of:
1. Nucleus pulposus
- A gelatinous core that contained hydrated gel, collagen fibres and elastin fibres
- Consists of hydrostatic pressure which maintains the consistency
- Function as a shock absorption system, dissipating and transferring load.
2. Annulus fibrosus
- A series of fibrous rings which made up from 50% – 60% of collagen fibers
- Provide strength and flexibility to the disc
.
Both of the disc material has the probability to be herniated. The herniation process begins as the nucleus pulposus start to lose its hydrostatic pressure and slowly bulge outward. For the annulus fibrosus, it begins from the failure in the innermost annulus rings and slowly progresses outward. It is most likely caused by the repeated or prolonged bending movement of the spine.
Types of herniated disc:
 |
Bulging: extension of the disc margin beyond the margins of the adjacent vertebral endplates |
 |
Protrusion:the posterior longitudinal ligament remains intact but the nucleus pulposus impinges on the anulus fibrosus |
 |
Extrusion:the nuclear material emerges through the annular fibers but the posterior longitudinal ligament remains intact |
 |
Sequestration: the nuclear material emerges through the annular fibers and the posterior longitudinal ligament is disrupted. A portion of the nucleus pulposus has protruded into the epidural space |
Risk factors:
-
Biomechanical factors:
Heavy working such as lifting heavy objects with bending trunk, pushing or pulling heavy objects are common factors to be associated with back pain or disc herniation. (McKenzie & May, 2003) A study reported that jobs involving heavy lifting while twisting the trunk with little bending of knees is even prone to disc prolapsed. This is due to the increased vertical loading and tension on annulus fibers while lifting and when the torsional load is added to this, the fibers are at a high risk to reach their tensile failure point. (Kelsey et. al, 1984)
Figure 1 clearly showed us that the lumbar intradiscal pressure increases when a person lifts a heavy object with bending trunk no matter in standing or seated position.
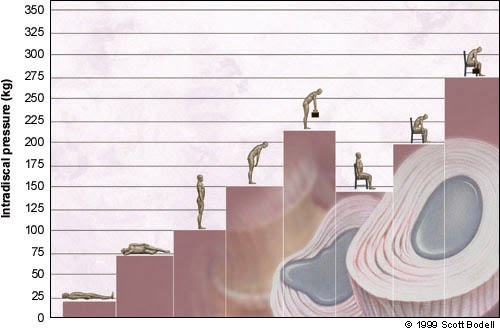
Figure 1: Postural changes have varying effects on the lumbar intradiscal pressure. In a normal upright standing position, 100kg of pressure is measured on the lumbar disc. However, when we are lifting heavy objects with a bending trunk, the pressure on the lumbar disc is increased up to 220kg. The highest pressure that is placed on the lumbar disc is the position of lifting heavy objects with the trunk leaning forward in a seated position.
.
Besides, biomechanical evidences showed that back and trunk muscles strength protects against spine and disc injuries. It is theorized that stresses in the disc are generally produced by intervertebral deformations, an increased muscle strength will make the intervertebral unit better able to cope with and therefore reduced the intervertebral deformities in response to suddenly applied overpressure in daily living. Hence, weak back and trunk muscles due to either sedentary lifestyle or soft tissue injuries can lead to disc herniation. (Mundt et. al, 1993) A sedentary lifestyle with prolonged static sitting position especially those office workers experienced increased lumbar intradiscal pressure (Figure 1) and this may exceed the stress tolerance of the disc, which will lead to the development of herniation. (Noguchi, 2013)

Figure 2: Different head positions have varying effects on the cervical intradiscal pressure.
For the cervical(neck), an increased spinal load will also increase the risk of cervical disc herniation. In a neutral head position looking straight ahead, 5kg of pressure is measured on the cervical disc. As the head tips forward, the pressure on the cervical disc will increase when the head gets further away from its neutral balance point as shown in Figure 2. For example, when you are looking down at a smartphone, the pressure on the cervical disc can be increased until 440%(27kg) and this will increase the risk of having cervical disc herniation.
-
Trauma
A herniated disc can be caused by injuries such as car accidents. For example, the sudden, jerking movement during accidents can put too much pressure on the disc and this will lead to herniation.
-
Obesity
Excess weight will alter the biomechanical changes in lumbar discs and joints, which may produce higher compressive force and pressure on the lumbar spine. This will increase the risk of lumbar disc herniation. (Sheng et. al, 2017)
-
Smoking
Cigarette smoke contains nicotine and more than 4000 other chemicals which will reduce the nutrient supply in vasculature and limit the blood flow. This will lead to a speeding up of disc degeneration and alterations of gross morphological structure of disc tissue, as well as cracks and disruption of annulus fibrosus, and eventually disc herniation might occured. (Jackson et. al, 2015)
Symptoms:
Lumbar slipped disc
-
Pain
Back pain onset is usually associated with bending, bending and lifting, or attempting to stand up after having been in a prolonged sitting or forward-bent posture. Normally, acute back pain lasts 3 to 4 weeks, while chronic back pain lasts longer than 3 months.
Back pain of slipped disc patients will be influenced by activity, position and movement. Normally, back pain may increase gradually when the patients have been in a prolonged sitting posture. Some activity like forward-bending and coughing will increase intradiscal pressure, hence aggravating back pain. Patients will feel symptoms reduced during standing and walking.
Patients with slipped discs may experience segmental or multi-segmental pain. Initially, patients feel pain in the lumbosacral or buttock region, slowly the aching may extend into the thigh. All the symptoms are variable depending on the degree and direction of protrusion as well as the spinal level of lesion. Back pain will slowly reduce after 12 months without any treatment, however the lesion wasn’t treated hence back pain easily recurring.
-
Paraesthesia or anesthesia
If the protrusion pressure is against the nerve roots or spinal cord, a patient may experience a sensation or a lack of sensation. Abnormal sensation include numbness, tingling, burning sensation and “pins and needles” feeling. Please be aware if you have abnormal sensations in the perineal area associated with urination problems. This is an emergency surgical situation because of potential long-term bowel and bladder problems if the pressure on the spinal cord is not relieved as soon as possible.
-
Weakness
Patients may notice that his/her legs have become weak or decrease in strength. This may be the result of an injury to the nerve supply.
-
Postural deviation
Patients may have some limitations or painful arch when moving the trunk. Trunk lateral deviation will be observed on patients with slipped discs due to avoiding the pain. Patients may side bend away from the painful side or bending towards the painful side depends on the degree and direction of the disc protrusion.
|
Postural Deviation |
||
| Away from the painful side
(Picture A) |
Protrusion is lateral to the nerve root. | |
| Towards the painful side
(Picture B) |
Protrusion is medial to the nerve root | |
| Alternating deviation | Small protrusion, on the midline. | |
| Deviation in standing, disappearing in full flexion | Small protrusion | |
| Deviation in full flexion | Small protrusion | |
| Deviation half way (painful arch) | Small protrusion | |


Cervical slipped disc
Symptoms of cervical slipped disc are similar to those in the lumbar spine. However, they are displayed in the respective dermatomes and myotomes of the cervical nerve roots. Symptoms may insidious onset after performing a relatively minor physical activity or maintaining a prolonged position. Initially, the patient may present with a faulty forward head posture and may hold the head in a guarded side bent or rotated position away from the symptomatic side. Neck forward bending peripheralizes the symptoms.There may be nerve mobility impairments in the upper extremity.

Dermatome of cervical
References:
-
Harada, A. et. al(1998). Correlation Between Bone Mineral Density and Intervertebral Disc Degeneration. Spine. 23(8). p. 857–861.
-
Jackson A. R. et. al (2015) Association Between Intervertebral Disc Degeneration and Cigarette Smoking: Clinical and Experimental Findings. JBJS Reviews. 3(3). p.1-9.
-
Kelsey J. L. et. al (1984). An Epidemiologic Study of Lifting and Twisting on The Job and Risk for Acute Prolapsed Lumbar Intervertebral Disc. Journal of Orthopaedic Research. 2(1). p. 61–66.
-
McKenzie R. and May S. (2003) The Lumbar Spine Mechanical Diagnosis & Therapy [Vol. 1]. p. 33-37.
-
Mundt D.J. et. al(1993). An epidemiologic study of sports and weight lifting as possible risk factors for herniated lumbar and cervical discs. The American Journal of Sports Medicine. 21(6). p. 854–860.
-
Noguchi M. (2013) Examining Changes in Intradiscal Pressure During Intervertebral Disc Herniation. University of Waterloo. p. 1-115.
-
Samini F. et. al (2014) The Etiologies of Low Back Pain in Patients With Lumbar Disk Herniation. Iran Red Crescent Med J. 16(10). p. e15670.
-
Sheng B. et. al (2017) Associations between Obesity and Spinal Diseases: A Medical Expenditure Panel Study Analysis. IJERPH. 14(2). p.183.