What is Cerebral Palsy?
Cerebral palsy (CP) is a group of permanent movement disorders and is a non-progressive brain disease. Cerebral palsy is mainly caused by abnormal development or damage to the brain cells that control movement early in life before or after birth. The muscle will receive abnormal instructions from the damaged or lesions part of the brain that impede muscle control, resulting in movement dysfunction due to stiffness or floppy of the muscle. Sometimes the damage affects other parts of the brain, which may cause difficulty with seeing, hearing, communicating and learning. However the damage to the brain does not get worse (non-progressive).
The prevalence rate of cerebral palsy is 2.4-3.6/1000, which is likely to occur in all types of families in any country. Although cerebral palsy cannot completely be cured by rehabilitation, it can help to reduce their dysfunction and maximize their potential. The effects of the rehabilitation depending on how soon the child starts the treatment and how damaged the brain is.
What causes Cerebral Palsy?
It can be roughly divided into: before birth, around the time of birth and after birth.
Before birth: Exposure to radiation, infection in the mother in the early weeks of pregnancy, for example German measles (rubella) or shingles, or uncontrolled diabetes and high blood pressure in the mother during pregnancy.
**With the development of science and technology, the radiation dose of x-ray has been reduced a lot. If pregnant women need to have x-ray examinations, they can request the value of the radiation dose from related staff and seek advice from obstetrician and gynecologist.
Around the time of birth: Some factors such as premature delivery, dystocia, birth injury (Forceps or Vacuum Extractor), double/ multiple births or nuchal cord etc., cause insufficient oxygen supply to the baby during or after delivery and lead to brain hypoxia
After birth: It may be caused by brain infections such as encephalitis, meningitis or head injuries, fever, physical illness, metabolic or endocrine abnormalities, and jaundice etc.
Types of Cerebral Palsy:
There are different motor performances and muscle tones depend on the part of the brain damaged. It can be roughly divided into spastic, athetoid, ataxic, hypotonia and mixed cerebral palsy. There are different treatment plans for different types of cerebral palsy.
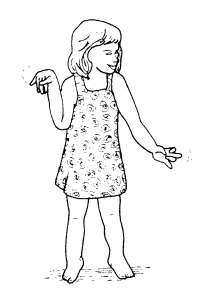
- Spastic: Approximately 77.4% of all cases. It can be classified into hemiplegia, diplegia and quadriplegia.
- Athetoid: 2.9%
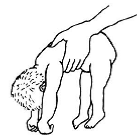
- Ataxic: 5.5%
- *Hypotonia*: A temporary transition stage before becoming spastic or athetoid
- Mixed: 14.2%. Show features of more than one type of cerebral palsy, for example: children have spastic cerebral palsy with athetoid movements.
|
Spastic |
|||
|
Site of injury |
Motor cortex of cerebral | ||
| Signs and symptoms |
|
||
|
Classification |
Hemiplegia |
Diplegia |
Quadriplegia |
|
Picture |
 |
 |
 |
|
Signs and symptoms |
Arm, body and leg were affected on one side, mainly the contralateral side of the brain was injured. Arm turned in and bent, hand fisted. Leg turned in and bent. Tiptoe standing. |
Legs affected more than arms. One or both arms are slightly clumsy. Legs pressed together and turned in. Tiptoe standing. |
Whole body is affected, usually arms affected more than legs or both are seriously affected. Poor head control, arms turned in and bent. Hand fisted. Leg pressed together and turned in. Tiptoe standing. |
|
Athetoid |
|
|
Site of injury |
Basal ganglia |
|
Picture |
 |
|
Signs and symptoms |
|
|
Ataxic |
|
|
Site of injury |
Cerebellum |
|
Picture |
 |
|
Sign and symptoms |
|
|
Hypotonia |
|
|
Picture |
 |
|
Sign and symptoms |
|
Mixed:
Show features of more than one type of cerebral palsy, for example some children have spastic cerebral palsy with athetoid movements.
Problems Found With Cerebral Palsy
- Vision problem – The most common problem is squint, but squints usually stop gradually as children get older. Children older than six months, with a squint, should be taken to an eye doctor because it may cause amblyopia in other eyes.
- Hearing problem – Cerebral palsy kids who have damaged hearing make learning to speak more difficult. If you suspect your kid has a hearing problem, please consult a doctor.
- Eating and speaking problem – Children can eat normally is an important preparation stage for learning to speak. So, if children have poor tongue, lips and throat muscle control, they may find difficulties in learning to chew and swallow. Hence, learning to speak can be delayed. Most of the cerebral palsy kids can speak but sometimes the words are not clear enough for others to understand. When this is so, more encouragement and opportunity should be given to the children.
- Growth problem – Children with eating difficulties may be slow to gain weight, so they may be thinner than usual. Some children do not develop their muscles due to lack of moving. Besides, children with hemiplegia, the affected arm and leg are usually thinner and shorter than the other arm and leg.
- Learning problem – About half of the cerebral palsy children’s learning abilities are normal, especially those with athetoid cerebral palsy, have average or good intelligence.
- Personality and behaviour problem – Cerebral palsy children may become more easily frustrated or angry when doing something due to having difficulty moving and communicating. They may also easily give up and not try. So it is important to encourage and understand them.
- Fits (Epilepsy) problem – Fits can start at any age but not all children are affected. Uncontrolled fits may damage the brain further and lower the child’s ability to learn. Fits can usually be controlled with medicine.–Mild fits: The child may stop what she is doing and stare without blinking. There may be some unusual movements, such as repeated movement of the lips or hands.
–Severe fits: The child may fall to the ground if she is standing or sitting. There will be strong uncontrollable jerking movements of her arms and legs, and loss of consciousness. Saliva will come out of her mouth and her eyes may roll up. Fits are usually short. Mild ones last only seconds, severe fits seldom last more than 10 to 15 minutes. Care of the child who is having a fit:- Move away from danger
- Loosen tight clothing
- Turn her onto one sight so that saliva can run out of her mouth and breathing is easier
- Stay with her until the fits stops and let he sleep , she may be drowsy when the fits stops
References: https://iris.who.int/bitstream/handle/10665/62696/WHO_RHB_93.1.pdf?sequence=1